Proforma for compassionate appointment in central govt
ANNEXURE
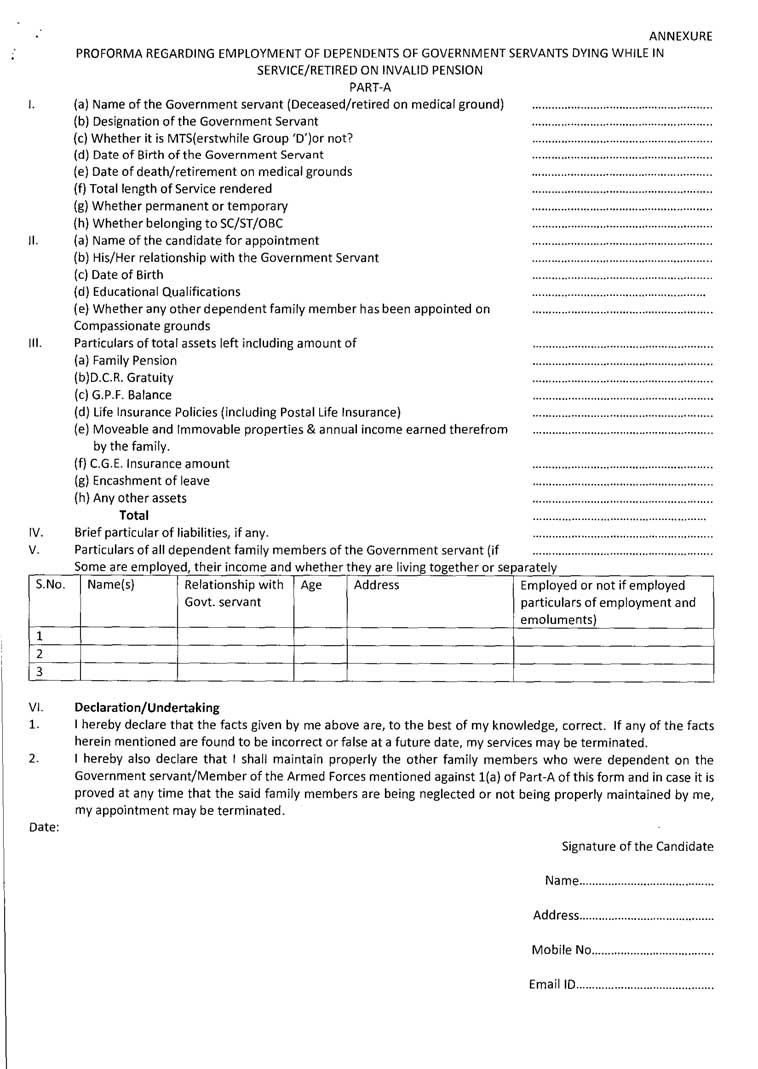
PROFORMA REGARDING EMPLOYMENT OF DEPENDENTS OF GOVERNMENT SERVANTS DYING WHILE IN SERVICE/RETIRED ON INVALID PENSION
PART-A
| I. | (a) | Name of the Government servant (Deceased/retired on medical ground) |
| (b) | Designation of the Government Servant | |
| (c) | Whether it is MTS(erstwhile Group ‘D’)or not? | |
| (d) | Date of Birth of the Government Servant | |
| (e) | Date of death/retirement on medical grounds | |
| (f) | Total length of Service rendered | |
| (g) | Whether permanent or temporary | |
| (h) | Whether belonging to SC/ST/OBC | |
| II. | (a) | Name of the candidate for appointment |
| (b) | His/Her relationship with the Government Servant | |
| (c) | Date of Birth | |
| (d) | Educational Qualifications | |
| (e) | Whether any other dependent family member has been appointed on compassionate grounds | |
| III. | Particulars of total assets left including amount of | |
| (a) | Family Pension | |
| (b) | D.C.R. Gratuity | |
| (c) | G.P.F. Balance | |
| (d) | Life Insurance Policies (including Postal Life Insurance) | |
| (e) | Moveable and Immovable properties & annual income earned therefrom by the family. | |
| (f) | C.G.E. Insurance amount | |
| (g) | Encashment of leave | |
| (h) | Any other assets | |
| Total | ||
| IV. | Brief particular of liabilities, if any. | — — — |
| V. | Particulars of all dependent family members of the Government servant (if Some are employed, their income and whether they are living together or separately.NoName(s)Relationship with Govt. servantAgeAddressEmployed or not if employed particulars of employment and emoluments)1.2.3. | |
| Vi. | Declaration/ Undertaking | |
| 1. | I hereby declare that the facts given by me above are, to the best of my knowledge, correct. If any of the facts herein mentioned are found to be incorrect or false at a future date, my services may be terminated. | |
| 2. | I hereby also declare that I shall maintain properly the other family members who were dependent on the Government servant/ Member of the Armed Forces mentioned against 1(a) of Part-A of this form and in case it is proved at any time that the said family members are being neglected or not being properly maintained by me, my appointment may be terminated. | |
| Date: | Signature of the Candidate | |
| Name | ||
| Address | ||
| Mobile No. | ||
| Email ID |

Leave a Reply